
Introduction
What causes the Indians to die and to diminish in number are secret judgments of God beyond the reach of Man. But what this witness has observed during the time he has spent in these parts is that from the province of Mexico have come three or four pestilences, on account of which the country has been greatly depopulated.
Pedro de Liévano, Dean of the Cathedral of Guatemala,
writing to the Council of the Indies (1582)
The outbreak, spread, and impact of Covid-19 is a harrowing reminder of how epidemic disease once wrought devastation on a scale unimaginable even by the uppermost levels of contagion and mortality of the pandemic that consumes us at present. Between 1346 and 1353, for instance, the Black Death (bubonic plague) that stalked Europe is reckoned to have killed an estimated 50 million, the Spanish Flu (H1N1 virus) between August 1918 and March 1919, eight horrific months, upward of 25 million worldwide [1]. Grim though the fatality figures for these two occurrences are, they are less than the number of Indigenous lives believed to have been lost in the Americas during the century following the Columbus landfall. We will never know precisely how many, but the deaths of 55 million Native Americans, some would argue more, cannot be ruled out [2]. While the turmoil of war and post-conquest exploitation abhorrent in the extreme took an immense toll, eruptions of sickness that autochthonous inhabitants had never been exposed to before are the most plausible explanation for the extent and severity of their demise [3].
Just as Covid-19 has stricken some countries or some regions within a country more than others, so too in colonial times did disease operate with notable spatial variation and long-term demographic fluctuation, east to west, south to north across the Americas. Period by period, place by place, no two experiences were exactly alike, local circumstances pertaining to environment, ecology, and culture differing markedly, and being affected likewise. The Taíno of Hispaniola – who greeted Columbus only to be spurned by him – have long since disappeared, the Beothuk of Newfoundland, the Yahi of California, and the Haush or Manek’enk of Tierra del Fuego along with them. In sharp contrast, Maya peoples to this day constitute close to half of Guatemala’s national population, which a government census in 2018 recorded as 14.9 million [4]. In the Guatemalan context, examining the relationship between epidemic incidence, native depopulation, and – in the case of the Sierra de los Cuchumatanes – eventual stabilization and survival affords a glimpse of what might be considered an optimal scenario, despite the iniquities still visited upon an Indigenous majority [5]. The Cuchumatán record, as is hoped soon too with Covid-19, also furnishes evidence of how a vaccine against infection can signal relief, evincing the difference between life and death, as it did in the region as the colonial era drew to a close.
Two objectives are in mind. The first, after setting the regional scene, is to review native population dynamics in the Sierra de los Cuchumatanes between the eve of Spanish arrival in Guatemala (1524) and Independence from Spain in 1821. Demographic decline from the early sixteenth century until three-quarters way through the seventeenth is linked to the ravages of epidemic disease, against which the region’s Maya peoples – like their counterparts across the Americas – were immunologically defenceless. Even after adjusting to the presence among them of introduced Old World infections, Indigenous inhabitants still proved acutely vulnerable when smallpox flared up again in the late eighteenth and early nineteenth centuries. The second objective is to reconstruct these particular episodes, for which data are rich and illuminating, to impart an idea of how utterly destructive pre-1780/1810 disease outbreaks must have been on native land and life.
The Regional Setting
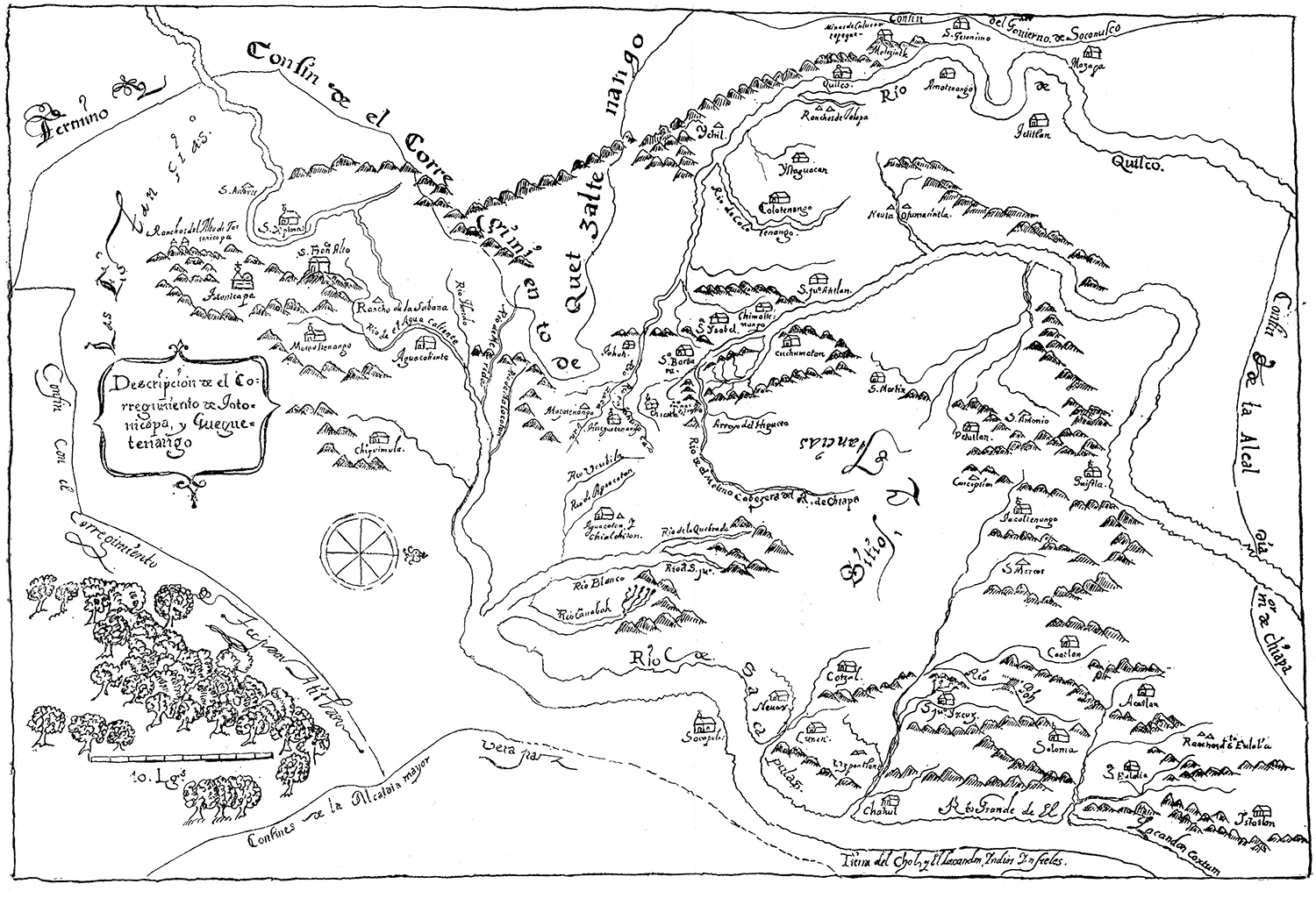
The Sierra de los Cuchumatanes is the most massive and spectacular non-volcanic region of all Central America. Lying to the north of the Río Cuilco, and to the north and west of the Río Negro or Chixoy, the Cuchumatanes form a well-defined unit bordered on the north by the tropical lowlands of the Usumacinta basin and on the west by the hilly Comitán country of the Mexican state of Chiapas. With elevations ranging from 500 to almost 3,900 metres, the region straddles the Guatemalan departments of Huehuetenango and Quiché, constituting some 15 percent (approximately 16,350 square kilometres) of the national territory (Figure 1).
According to a census conducted in 2002, Guatemala supported a population of 11.2 million, 41 percent of whom were considered Indigenous. Non-indigenous persons of mixed ancestry, referred to as Ladinos, made up the majority of the remainder. In the mountain areas north and west of the capital, Guatemala City, Indigenous communities predominate. Highland Guatemala, therefore, can in large measure be considered Indigenous Guatemala, home to some twenty Maya ethnicities in all. The 2002 census, the eleventh to be conducted at national level since 1778, recorded the Cuchumatán population at 1.05 million, of whom 742,284, roughly three out of four, were considered Indigenous. While the total Cuchumatán population doubled in the thirty years after the 1973 census, the Indigenous to non-Indigenous ratio remained the same [6]. Native peoples in the Cuchumatanes belong to several closely related but distinct Maya-language groups, the most important of which are Akateko (Jakalteko), Awakateko, Chuj, Ixil, Q’anjob’al, Mam, K’iche’, and Uspanteko.
Indigenous Population Dynamics, 1520-1821
Any attempt to reconstruct Cuchumatán population history is beset by a lack of consistent, representative data. Paucity of sources is most problematical for the sixteenth and seventeenth centuries; the eighteenth, by comparison, is well documented. Estimates of Indigenous numbers between first contact with Spanish or Spanish-led invaders in the 1520s and gaining independence from Spain in 1821 are shown in Table 1.
Table 1. The Indigenous Population of the Cuchumatán Highlands (1520–1825)
|
Year |
Population |
Comments and source |
|
1520 |
260,000 |
Extrapolation from the size of Indian armies recorded by Fuentes y Guzmán in the Recordación florida (1690–99). |
|
1525–30 |
150,000 |
Estimate based on the size of Indian armies recorded by Fuentes y Guzmán in the Recordación florida (1690–99). |
|
1550 |
73,000 |
Estimate based on figures for Huehuetenango in AGI, AG 10 and AGCA, A3.16, leg. 1601, exp. 26391. |
|
1578–82 |
47,000 |
Estimate based on figures for Huehuetenango in AGI, AG10 and AGCA, A3.16, leg. 1601, exp. 26391. |
|
1664–78 |
16,162 |
Based on comprehensive tribute assessments in AGCA, A3.16, leg. 1601, exp. 26391. |
|
1683 |
16,000 |
Estimate based on partially destroyed regional census in AGI, Contaduría 815. |
|
1690 |
19,258 |
Based on tribute data compiled by Fuentes y Guzmán in the Recordación florida (1690–99). |
|
1710 |
18,000 |
Estimate based on figures of the servicio del tostón for Totonicapán and Huehuetenango in AGI, Contaduría 973. |
|
1719 |
17,500 |
Estimate based on figures of the servicio del tostón for Totonicapán and Huehuetenango in AGI, Contaduría 977. |
|
1724 |
18,500 |
Estimate based on figures of the servicio del tostón for Totonicapán and Huehuetenango in AGI, Contaduría 976. |
|
1760 |
21,176 |
Based on comprehensive tribute assessments in AGCA, A3.16, leg. 950, exp. 17715. |
|
1768–70 |
23,418 |
Based on a head count recorded by Cortés and Larraz in his Descripción geográfico-moral de la diócesis de Goathemala (1768–70). |
|
1778 |
27,505 |
Based on head count in AGCA, A1.44, leg. 6097, exp. 55507. |
|
1779 |
28,047 |
Based on head count in AGCA, A1.44, leg. 6097, exp. 55507. |
|
1782 |
23,021 |
Based on head count in AGCA, A1.44, leg. 6097, exp. 55507. |
|
1783 |
25,027 |
Based on head count in AGCA, A1.44, leg. 6097, exp. 55507. |
|
1784 |
24,828 |
Based on head count in AGCA, A1.44, leg. 6097, exp. 55507. |
|
1788 |
24,678 |
Based on comprehensive tribute assessments in AGCA, A3.16, leg. 246, exp. 4912. |
|
1790 |
23,623 |
Based on detailed population and tribute data in AGCA, A3.16, leg. 237, exp. 4706. |
|
1797–98 |
24,129 |
Based population and tribute data recorded by Joseph Domingo Hidalgo in the Gazeta de Guatemala. |
|
1801 |
27,477 |
Based on detailed population and tribute data in AGCA, A3.16, leg. 243, exp. 4853. |
|
1811 |
29,571 |
Based on comprehensive tribute assessments in AGCA, A3.16, leg. 953, exp. 17773. |
|
1825 |
34,691 |
Based on population data in AGCA, B84.3, leg. 1135 and 1136, exps. 26030, 26031, 26032, and 26034. |
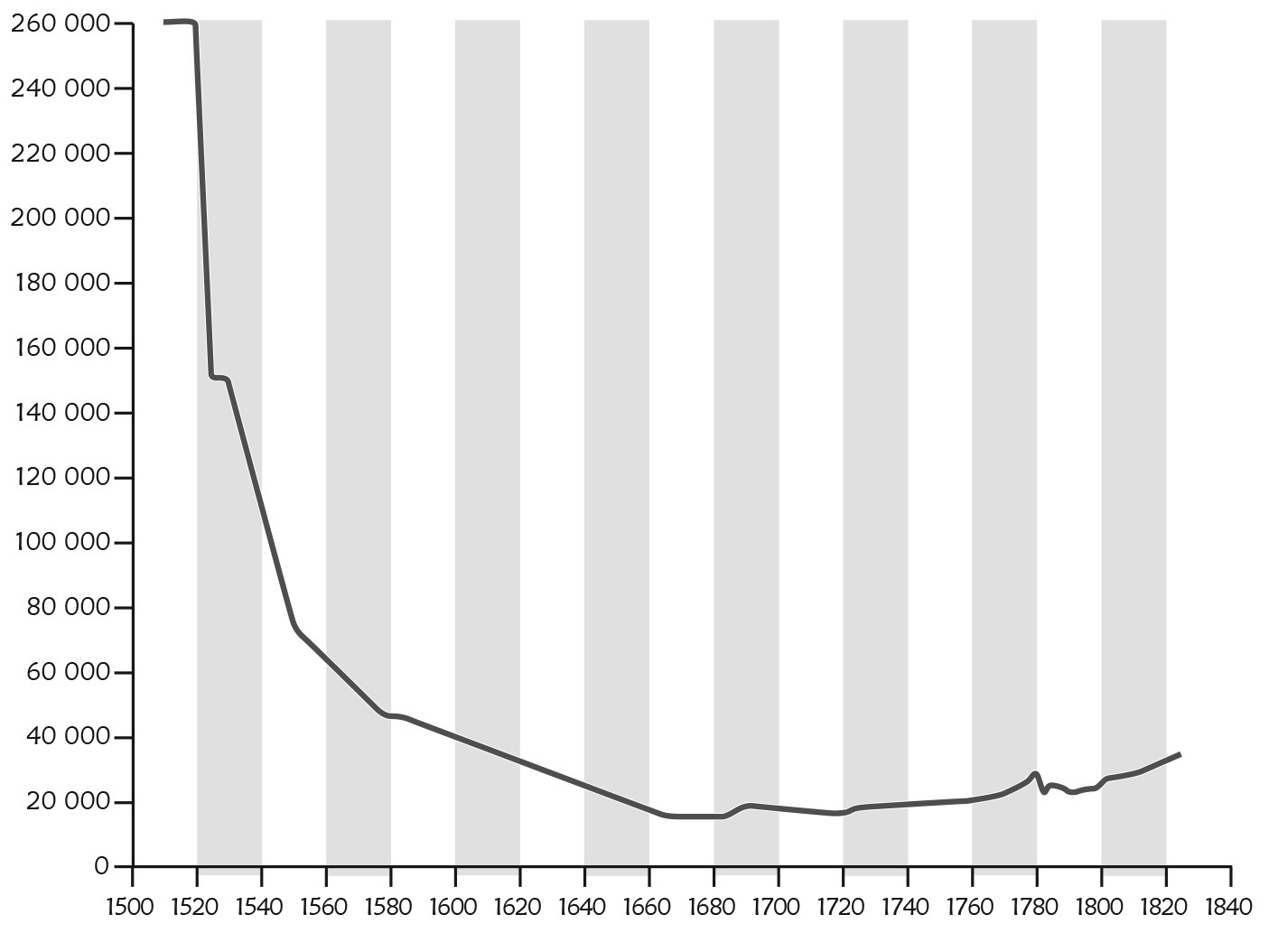
The most compelling feature of Cuchumatán population history is the catastrophic decline in numbers that followed conquest by Spain. Precipitous collapse began in the years immediately preceding Spanish intrusion and plummeted throughout the sixteenth and well into the seventeenth century. Reaching its nadir around 1680, the native population thereafter began to stabilize and rebound, though downturns still occurred. The three-century-long dynamic is plotted in Figure 2. By the start of the nineteenth century, Indigenous numbers embarked on an upward trend, which accelerated in pace in the course of the twentieth century.
Epidemic Disease and Demographic Crisis
The factors responsible for population collapse, stabilization, and fluctuating recovery are complex. Within the lethal mix that accounts for decline, especially during the sixteenth century, epidemic disease is paramount. Prior to Old World contact with the New, Native Americans enjoyed an existence relatively free of severe infectious contagions, being prone primarily to gastro-intestinal and respiratory disorders. Woes such as measles, mumps, smallpox, and typhus – all endemic to the Old World – were unknown. When these maladies entered the “virgin soil” environments of the Americas, their combined impact resulted in unprecedented loss of life.
The first disease to arrive was smallpox. Scrutiny by Juan Gil and Consuelo Varela of a log by Columbus establishes its presence on Hispaniola as early as 1493, linked to a Taíno native returning to his island home on the Admiral’s second voyage [7]. Two decades later smallpox was the scourge of Mexico, the Franciscan friar known as Motolinía documenting its devastation, as did also an array of Indigenous commentators [8]. The disease continued its destructive passage south toward Guatemala, accompanied perhaps by pulmonary plague or typhus [9]. As 1520 drew to a close, four years before the arrival of forces led by Pedro de Alvarado, Maya peoples in Guatemala were reeling from their exposure to what Murdo MacLeod aptly calls “the shock troops of the conquest” [10]. Indigenous Kaqchikel chroniclers lament that it was “in truth terrible, the number of dead among the people [...] in that period [...] when the plague raged” [11]. In Guatemala, this initial bout of pestilence was followed twelve years later by an outbreak of measles [12]. Thereafter, surges of disease were a common occurrence (Table 2). As well as being struck by epidemics of far-flung pandemic proportion, Cuchumatán communities also had to contend with more localized episodes (Table 3).
Table 2. Widespread Outbreaks of Disease in Highland Guatemala (1519–1746)
|
Year |
Disease |
Impact |
|
1519–20 |
Smallpox and perhaps also pulmonary plague or typhus |
Very high mortality; at least one-third of the Indian population would have perished |
|
1532–34 |
Sarampión (measles) |
High mortality among Indians |
|
1545–48 |
Gucumatz (a type of plague); peste (unspecified sickness) |
Very high mortality among Indians |
|
1563–65 |
Unspecified epidemic preceded by drought and famine |
– |
|
1571 |
Peste (unspecified sickness) |
– |
|
1576–77 |
Peste, viruela (smallpox), matlazáhuatl (typhus?), and gucumatz |
High mortality among Indians; several more settlements entirely depopulated |
|
1600–01 |
Smallpox (?) |
– |
|
1607–08 |
Tabardillo (typhus and/or a type of plague) |
Disease only affected Indians; Spaniards untouched |
|
1614 |
Unspecified epidemic |
Illness confined to Indians |
|
1631 |
Tabardillo (typhus) |
Many deaths among Indians |
|
1650 |
Gucumatz, bubonic plague |
Many deaths; villages depopulated |
|
1666 |
Peste, tabardillo |
Many deaths |
|
1686 |
Typhus and/or pneumonic plague |
High mortality among Indians and the poor |
|
1693–94 |
Sarampión, viruela, tabardillo |
High mortality |
|
1695 |
Smallpox |
– |
|
1704-05 |
Peste |
– |
|
1708–09 |
Peste |
Only Indians affected |
|
1710–11 |
Peste |
Some villages completely depopulated |
|
1733 |
Peste, smallpox, typhoid |
Many deaths |
|
1741 |
Tabardillo |
– |
|
1746 |
Tabardillo |
– |
Source: MacLeod (1973) 2008, 98–100.
From the 1520s until the end of Spanish rule in 1821, the Sierra de los Cuchumatanes was lashed by unrelenting waves of sickness. Rates of mortality varied but were consistently high. Between 1520 and 1683, Indigenous numbers in the region fell by more than 90 percent, from perhaps 260,000 to a low of about 16,000. That downward spiral abated by the end of the seventeenth century, when the first signs of recovery are manifest. Several fluctuations in the course of the eighteenth century, however, indicate ongoing vulnerability, to smallpox in particular. Only at the very end of the colonial period are there signs of a sustained increase in native numbers across the region as a whole.
Guatemalan and Spanish archives house a bounty of documents that describe, often in lugubrious detail, the desolation that was caused. In an attempt to convey a nuanced sense of it, we now turn to examining outbreaks of smallpox between 1780 and 1810. While a focus on these three decades, and that particular malady, is dictated by the availability of data, by all accounts the events and circumstances described apply also to earlier disease incidents and crisis situations.
Table 3. Local Outbreaks of Disease in the Cuchumatán Highlands (ca 1550–1819)
|
Year |
Disease |
Communities affected |
Comments |
Source |
|
1550–ca 1615 |
Pestes (unspecified sickness) |
Aguacatán and other settlements in the “sierra de Cuchumatán” |
The source records specifically that “con las pestes han venido [los pueblos] en diminución.” |
Remesal, Historia General (1619) |
|
1552 |
Unspecified |
Aguacatán and other towns |
The source states that “los pueblos han venido en gran descrecimiento y disminución” and that “se han muerto e ido de ellos otra mucha más cantidad.” |
AGI, Justicia 286 |
|
1568 |
Unspecified |
Aguacatán, Sacapulas, and two other towns held in encomienda by Alonso Páez |
Because of Indian population decline, the income accruing to the encomendero is expected to total less than 100 pesos. |
AGI, Patronato 68-2-3 |
|
1571 |
Unspecified |
Sacapulas region |
The same disease struck communities in the Verapaz, with considerable mortality. |
AGCA, A1, leg. 5942, exp. 51995 |
|
1582 |
Unspecified |
Chiantla, Huehuetenango “y sus estancias” |
The source records that “los indios han venido en diminución, la encomienda ha venido a menos.” |
AGI, Patronato 61-2-4 |
|
1613 |
Unspecified |
Todos Santos Cuchumatán |
The tribute assessment has been lowered “por falta de tributarios.” Mention is made of “indios viejos y enfermos.” |
AGI, Patronato 58-1-4 |
|
1617 |
Unspecified |
San Martín Cuchumatán |
The source mentions “indios enfermos.” |
AGI, Patronato 58-1-5 |
|
1639 |
Peste (unspecified sickness) |
La Magdalena, near Cunén, and Sacapulas |
The source refers to “una formidable peste.” The people who survived the epidemic were resettled in Cunén and Sacapulas, forming in the latter the parcialidad Magdalena. |
AGCA, A1, leg. 6037, exp. 53258 |
|
1666 |
Tabardillo (typhus) |
Huehuetenango |
Indian tribute lowered after epidemic carried off 45 adults. |
AGCA, A3.16, leg. 1600, exp. 26390 |
|
1733 |
Viruela (smallpox) |
Cunén and Sacapulas |
Many tributaries died. The Indians, unable to pay tribute, request an exemption. |
AGCA, A3.16, leg. 2819, exp. 40918 |
|
1774 |
Peste (unspecified sickness) |
Various towns in Totonicapán and Huehuetenango |
The alcalde mayor informs treasury officials that, because of the pestilence, certain communities are unable to pay tribute. |
AGCA, A3.16, leg. 943, exp. 17608 |
|
1780–81 |
Viruela |
Every major settlement in the Cuchumatán region |
Over 4,000 deaths among the Indians. Children were particularly hard hit by the epidemic, thought to have originated in Chiapas. |
AGCA, A1.44, leg. 6097, exp. 55507 |
|
1786 |
Tabardillo |
Concepción and Petatán |
The sickness is recorded as having broken out on September 2. |
AGCA, A1.4, leg. 6101, exp. 55666 |
|
1795 |
Viruela |
Towns along the camino real and throughout Soloma parish |
The disease is thought to have spread east and south from Chiapas. |
AGCA, A1.47, leg. 385, exp. 8012 |
|
1796–99 |
Tabardillo |
Various towns, especially those in the parishes of Huehuetenango, Jacaltenango, and Nebaj |
Very high mortality. In San Sebastián Huehuetenango, over 1,000 Indians perished. An equal number died in Concepción and Jacaltenango. |
AGCA, A1.24, leg. 6101, exp. 55666-9; AGCA, A1.49, leg. 192, exp. 3911; AGCA, A3, leg. 2894, exp. 42846; AGCA, A3.16, leg. 244, exp. 4869; AGCA, A3.16, leg. 255, exp. 5719 |
|
1802–07 |
Tabardillo |
Towns throughout Soloma parish |
Considerable mortality. Settlements abandoned, fields neglected, and normal life totally disrupted. Locust invasion exacerbates crisis. Great misery. |
AGCA, A1, leg. 6105, exp. 55795; AGCA, A1, leg. 6107, exp. 55836; AGCA, A1. 24, leg. 6091, exp. 55306; AGCA, A1.47, leg. 2162, exp. 15558; AGCA, A3.16, leg. 245, exp. 4909 |
|
1803–07 |
Viruela |
Numerous towns, including Soloma, Santa Eulalia, and San Juan Ixcoy |
Smallpox prevails, despite efforts by Spanish authorities to vaccinate the Indians. |
AGCA, A1.4, leg. 6091, exp. 55307; AGCA, A1.47, leg. 2162, exp. 15558-9; AGCA, A1.47, leg. 192, exp. 3922 |
|
1804–05 |
Sarampión (measles) |
Chiantla and the towns of Soloma parish |
Disease probably originated in Chiapas. |
AGCA, A1, leg. 6091, exp. 55307; AGCA, A3.16, leg. 2899, exp. 43063 |
|
1811 |
Fiebre putrida (a type of fever) |
Various communities throughout Totonicapán and Huehuetenango |
Doctors request permission to draw money from community funds to help fight the spread of sickness. |
AGCA, A1, leg. 394, exp. 8238 |
|
1812 |
Peste (unspecified) |
Chajul and San Juan Cotzal |
The Indians are unable to pay tribute because of disease-related mortality. |
AGCA, A3.16, leg. 2900, exp. 43154 and 43178 |
|
1812–14 |
Tabardillo |
Chiantla, San Juan Cotzal, and the towns of Soloma parish |
Roads into the infected communities are ordered closed and a “cordón sanitario” is set up. |
AGCA, A1.4, leg. 386, exp. 8055; AGCA, A1.4, leg. 6114, exp. 56316; AGCA, A1.4, leg. 6116, exp. 56424 |
|
1818–19 |
Tabardillo |
Chiantla and Jacaltenango |
Religious festivities are to be cancelled because of the prevailing sickness. |
AGCA, A1.4, leg. 388, exp. 8099; AGCA, A1.4, leg. 6118, exp. 56743 |
Table 4. Mortality in Cuchumatán Towns during the Smallpox Epidemic of 1780–81
|
Community |
Married Males |
Married Females |
Widowers |
Widows |
Single Males |
Single Females |
Boys |
Girls |
Total no. of dead |
No. of dead Tributaries |
Indian Population in 1779 |
% Mortality |
|
Aguacatán and Chalchitán |
5 |
10 |
– |
– |
18 |
12 |
49 |
43 |
137 |
5 |
904 |
15 |
|
Amatenango |
2 |
2 |
4 |
– |
3 |
4 |
9 |
12 |
36 |
2 |
186 |
19 |
|
Colotenango |
10 |
15 |
3 |
4 |
27 |
8 |
31 |
42 |
140 |
15 |
1,042 |
13 |
|
Concepción |
7 |
17 |
– |
2 |
22 |
14 |
44 |
41 |
147 |
7 |
480 |
31 |
|
Chajul |
5 |
15 |
– |
– |
10 |
– |
86 |
77 |
195 |
5 |
1,358 |
14 |
|
Chiantla |
6 |
8 |
– |
2 |
13 |
7 |
20 |
7 |
63 |
5 |
225 |
28 |
|
Cuilco |
1 |
2 |
– |
1 |
7 |
7 |
23 |
14 |
55 |
3 |
304 |
18 |
|
Cunén |
16 |
20 |
7 |
1 |
3 |
2 |
12 |
16 |
77 |
10 |
244 |
32 |
|
Huehuetenango |
5 |
6 |
1 |
1 |
15 |
17 |
20 |
15 |
80 |
6 |
602 |
13 |
|
Ixtahuacán |
9 |
30 |
4 |
4 |
15 |
23 |
45 |
43 |
173 |
12 |
947 |
18 |
|
Jacaltenango |
13 |
28 |
4 |
1 |
32 |
29 |
80 |
86 |
273 |
15 |
1,728 |
16 |
|
Malacatán |
2 |
4 |
2 |
3 |
2 |
4 |
9 |
9 |
35 |
2 |
180 |
19 |
|
Nebaj |
6 |
11 |
– |
– |
19 |
15 |
58 |
56 |
165 |
7 |
1,428 |
12 |
|
Sacapulas |
14 |
42 |
11 |
9 |
21 |
24 |
78 |
101 |
300 |
10 |
1,906 |
16 |
|
San Andres |
1 |
8 |
– |
– |
8 |
5 |
19 |
13 |
49 |
1 |
294 |
17 |
|
San Antonio Huista |
10 |
1 |
– |
– |
1 |
6 |
3 |
11 |
32 |
6 |
136 |
24 |
|
San Francisco |
– |
3 |
– |
2 |
3 |
3 |
7 |
12 |
30 |
1 |
125 |
24 |
|
San Gaspar Ixchil |
– |
– |
1 |
1 |
3 |
3 |
5 |
8 |
21 |
1 |
273 |
8 |
|
San Juan Atitán |
1 |
13 |
1 |
3 |
10 |
4 |
29 |
35 |
96 |
2 |
473 |
17 |
|
San Juan Cotzal |
11 |
17 |
– |
– |
8 |
3 |
48 |
47 |
138 |
11 |
1,707 |
8 |
|
San Juan Ixcoy |
5 |
9 |
– |
1 |
21 |
24 |
35 |
39 |
154 |
6 |
934 |
16 |
|
San Lorenzo |
4 |
7 |
– |
– |
2 |
2 |
11 |
11 |
37 |
4 |
330 |
11 |
|
San Marcos |
8 |
6 |
– |
– |
7 |
– |
11 |
21 |
53 |
8 |
228 |
18 |
|
San Martín |
– |
1 |
– |
– |
1 |
3 |
10 |
9 |
24 |
– |
118 |
20 |
|
San Martín Mazapa |
1 |
1 |
– |
3 |
10 |
4 |
4 |
19 |
42 |
3 |
208 |
26 |
|
San Mateo Ixtatán |
10 |
26 |
20 |
6 |
32 |
10 |
55 |
72 |
231 |
12 |
1,132 |
20 |
|
San Miguel Acatán |
5 |
12 |
1 |
5 |
31 |
18 |
24 |
33 |
129 |
5 |
338 |
38 |
|
San Pedro Necta |
3 |
8 |
1 |
– |
11 |
5 |
26 |
13 |
67 |
3 |
527 |
13 |
|
San Sebastián Coatán |
8 |
11 |
– |
– |
13 |
14 |
26 |
51 |
123 |
8 |
463 |
27 |
|
San Sebastián |
6 |
16 |
– |
2 |
43 |
43 |
74 |
68 |
252 |
6 |
2,275 |
11 |
|
Santa Ana Huista |
8 |
10 |
– |
2 |
11 |
7 |
11 |
4 |
53 |
7 |
395 |
13 |
|
Santa Bárbara |
3 |
2 |
– |
– |
10 |
3 |
15 |
17 |
50 |
3 |
386 |
13 |
|
Santa Eulalia |
19 |
37 |
3 |
3 |
31 |
28 |
84 |
92 |
297 |
17 |
1,577 |
19 |
|
Santa Isabel |
2 |
3 |
1 |
– |
12 |
16 |
11 |
11 |
56 |
3 |
532 |
11 |
|
Santiago |
2 |
1 |
– |
3 |
7 |
14 |
28 |
24 |
79 |
2 |
484 |
16 |
|
Petatán |
9 |
– |
2 |
1 |
1 |
– |
4 |
– |
17 |
9 |
94 |
18 |
|
Soloma |
5 |
5 |
2 |
1 |
2 |
3 |
7 |
17 |
42 |
5 |
285 |
15 |
|
Tectitán |
5 |
6 |
– |
1 |
12 |
8 |
30 |
13 |
75 |
4 |
275 |
27 |
|
Todos Santos |
1 |
8 |
– |
1 |
12 |
10 |
36 |
38 |
106 |
– |
721 |
15 |
|
Uspantán |
11 |
22 |
5 |
2 |
22 |
3 |
10 |
11 |
86 |
22 |
361 |
24 |
|
4,215 |
253 |
After reaching its nadir of 16,000 around 1680, the Cuchumatán population increased in size, albeit slowly, for the next one hundred years. By 1779, it had risen about 75 percent above the estimate calculated for 1683, numbering slightly over 28,000. The vast majority of this population was Indigenous; Ladinos and Spaniards accounted for only 5 percent of the regional total at the end of the colonial period, and constituted an even smaller percentage during earlier times. Demographic recovery between 1683 and 1779, therefore, was an overwhelmingly native phenomenon, though castas (people of mixed race) were by then a conspicuous presence in certain towns and parts of the countryside [13]. With the onset in 1780 of a virulent outbreak of smallpox, one that can be considered but a regional manifestation of a hemispheric pandemic, the upward trend was abruptly arrested [14].
Smallpox is documented as having been in existence on March 28, 1780 in San Martín Mazapa and San Francisco Motozintla, communities in the westernmost part of the parish of Cuilco, today located in Chiapas, Mexico. A priest named Manuel Ordóñez noted the date, the earliest recorded occurrence [15]. The epidemic persisted in the region, notably in San Lorenzo Mazatenango, at least until January 1781, nine months later. In some communities (San Martín Mazapa and San Francisco Motozintla, for example) smallpox raged for four months; others (for example, Santiago Chimaltenango and San Sebastián Huehuetenango) endured the pestilence one or two months longer. In Asunción Colotenango, smallpox lingered for fully seven months (see Figure 3). The chronology of recorded incidence suggests a rapid spread of infection east from a location in Chiapas along the southern edge of the Cuchumatanes (possibly by way of the Cuilco valley) with a slower diffusion north into higher and more remote parts of the region [16].
In response to a request of his, Francisco Geraldino, governor of the province of Totonicapán and Huehuetenango, received from priests like Ordóñez data concerning the number of deaths that could be attributed to smallpox [17]. Geraldino, acting on royal orders, then gathered parish statistics together, completing the task on May 2, 1781. His responsibility appears to have been twofold: first, he was to determine how many of the dead were tribute payers, an exercise undertaken to assess how taxes levied on smitten communities would in the immediate future be taken into account; second, he was to determine which towns were most in need of assistance, and act accordingly. Geraldino synthesized the information relayed to him – some priests were more assiduous in furnishing data than others – in a table he called a “general summary showing mortality related to the smallpox epidemic of 1780, with a listing of the number of deceased tributaries and the amount [of money] with which communities were assisted” [18]. A detailed town-by-town breakdown of the impact of the epidemic, based on Geraldino’s summary, is shown in Table 4.
Over 4,000 natives of all ages perished, with almost 60 percent of total recorded deaths occurring among children [19]. Of those who died, 259 were reported by Geraldino to have been tribute payers. Only one priest, Fray Juan Ramón Solís of the parish of Nebaj, provided Geraldino with specific details about the number of people who not only died from smallpox but who fell sick with fever and were nursed back to health [20]. This information enables some assessment to be made of the degree of infection and the rate of survival or recovery. The data are shown in Table 5 and relate to the three Ixil Maya communities of San Gaspar Chajul, San Juan Cotzal, and Santa María Nebaj. Some idea of how disruptive the epidemic must have been of such routine chores as tending fields, fetching water, or preparing food is indicated by Ramón Solís reporting that, in San Gaspar Chajul, three out of every five people fell ill. Of those laid low, one in four perished, a pattern that holds also for the neighbouring communities of San Juan Cotzal and Santa María Nebaj.
Table 5. Extent of Infection, Recovery, and Fatality during the Smallpox Epidemic of 1780 in Ixil Country
|
A Community |
San Gaspar Chajul |
San Juan Cotzal |
Santa María Nebaj |
|
B Population in 1779 |
1358 |
1707 |
1428 |
|
C No. of People Afflicted by Smallpox in 1780 |
836 |
503 |
614 |
|
D C as % of B |
62 |
29 |
43 |
|
E No. of Smallpox Deaths in 1780 |
195 |
138 |
165 |
|
F |
23 |
27 |
27 |
Source: AGCA, A1.24, leg. 6097, exp. 55507.
Mortality rates varied considerably, from 8 percent in San Gaspar Ixchil to 38 per cent in San Miguel Acatán, indicating significant spatial variation (see Figure 4) in the impact of the epidemic, some pueblos de indios being much harder hit than others (Table 4). Assuming it was the same strain of smallpox that was involved, differences in disease impact most likely were caused by a combination of factors, including demographic composition; population density; degree of settlement nucleation or dispersal; extent of previously acquired immunity; level of pre-contagion health and nutrition; effectiveness of quarantine procedures; proximity to routes of trade and communication; and numerous cultural and environmental characteristics relating to habit and habitat [21]. In other words, variable local conditions that changed in myriad ways from valley to valley, from town to town, best account for differences in mortality. Within a year the epidemic had reduced the population of the region, after a century or so of gradual recovery, from 28,000 to around 24,000, a drop of almost 15 percent.
On August 29, 1780, authorities began to respond to the crisis. Geraldino issued a rather vague precautionary order stating that “the Indians should be cared for and assisted by drawing upon the resources of their communities” [22]. Following an inspection of several towns, officials made recommendations about what could be done to alleviate the situation, above all to halt the spread of disease. Most of these amounted to little more than allocating certain towns a sum of money withdrawn from their own community funds. This money was then spent on bedding, clothing, and food – and in administering the holy sacraments to the dead [23]. Parish priests were responsible for distributing goods and provisions, dispatched from Huehuetenango, among those families considered most in need. In Aguacatán and Chalchitán the sum of ten pesos bought a quantity of sugar and thirty-eight woven mats for people to sleep on; in Todos Santos, twenty pesos purchased sugar, ten woven mats, and cloth used to make blankets [24]. Financial assistance seems only to have been extended to eleven towns, most communities left to fight the sickness with their own limited resources. Though Francisco Asturias, in his history of Guatemalan medicine, records inoculation as having been carried out during this epidemic, just how extensive the practice was in the Sierra de los Cuchumatanes is a matter of conjecture [25].
By early 1781 the epidemic that had begun a year or so before had run its course. Within ten years the tribute payers in the province of Totonicapán and Huehuetenango attained pre-contagion numbers. Total population, however, did not reach pre-contagion levels for another decade [26]. A less intense, more localized outbreak of smallpox flared up again in 1795 and 1796 [27]. Joseph Domingo Hidalgo, a Crown official and a contributor to the Gazeta de Guatemala, wrote positively about efforts to control the spread of infection:
In 1795 and 1796 the towns that border the province of Chiapas [...] were overrun by a terrible outbreak of smallpox, an all-consuming pestilence that has plagued this Kingdom of Guatemala throughout the 275 years it has been conquered by Spain, destroying generation after generation, leaving barely one-tenth of the [contact] population alive. On this occasion, however, due to the efforts of Don José Domás y Valle, president and captain general of the Kingdom, the outbreak was isolated, procedures of inoculation were set up, and the pestilence was stamped out at the peak of its virulence. [28]
About a dozen towns were hit by this outbreak, all of them lying to the north and west of Huehuetenango, with the eastern Cuchumatanes apparently left untouched and unharmed. Specific reference is made about the coldness, remoteness, and general environmental inhospitality of the region being among the “physical causes” of the resurgence, with the authorities admitting that rugged terrain would hamper relief operations, even if they were attempted in the first place [29].
The outbreak of 1795–96 was followed, seven years later, by yet another appearance of smallpox, once again focused on the border area with Chiapas [30]. Although this outbreak was less serious than those of 1780–81 and 1795–96, the authorities reacted (perhaps because of the impact of the earlier visitations) with stronger emergency measures, including inoculation and quarantine [31]. Since many of the towns where smallpox reappeared were located on the highway (camino real) between Mexico and Guatemala – Chiapas was the actual or perceived origin of many diseases that ravaged the Sierra de los Cuchumatanes throughout the colonial period – this main thoroughfare was ordered closed [32]. A garita or control point at either San Antonio or Santa Ana Huista was set up to ensure that trade and journeys originating in neighbouring Mexico with an eventual Guatemalan destination were monitored. Theoretically, restrictions were placed on the movement of people and goods early in December 1802, but enforcement was lax; one official alleged that the watch was anything but vigilant, remarking that “people have come, and come still, increasingly from all parts” [33]. Commerce and the exercise of personal convenience – as with Covid-19 in our day – often made quarantine an impractical charade, at the Huistas and elsewhere.
Table 6. Vaccination against Smallpox among Cuchumatán Indians (1807)
|
Parish |
Number of Indians Vaccinated |
Cost of Vaccination |
|
Chiantla |
515 |
64 pesos 3 reales |
|
Jacaltenango |
762 |
95 pesos 2 reales |
|
Malacatán |
621 |
77 pesos 5 reales |
|
Nebaj |
348 |
43 pesos 4 reales |
|
Soloma |
1,186 |
148 pesos 2 reales |
Source: AGCA, A1.47, leg. 2162, exp. 15558.
Vaccine and Vindication
By the early nineteenth century, however, a development had taken place that was to alter irrevocably the relationship between smallpox and humankind, with considerable potential benefits for Indigenous communities like those of the Sierra de los Cuchumatanes. In 1798, Edward Jenner, an English country doctor, published his findings concerning inoculation against smallpox, documenting his observation that milkmaids seemed never to succumb to smallpox because, as he correctly hypothesized, they had developed an immunity to the disease by first contracting cowpox. Subsequent inoculation of human patients with cowpox matter, the medical risks of which were negligible, demonstrated that immunity to smallpox did in fact occur, thus establishing “vaccination” as the definitive preventative measure against the disease [34].
Word of Jenner’s breakthrough spread throughout Europe, and in Spain was responsible for the setting up of a medical mission to circulate news of “the fortunate English discovery” [35] throughout Spanish America. Headed by Doctor Francisco Xavier de Balmis, the mission set sail from the port of La Coruña on November 30, 1803, bound for Mexico (and the Philippines beyond) with the enlightened objective of informing local doctors of Jenner’s successful experiments in establishing immunity against smallpox by means of vaccination [36].
Francisco Pastor, a member of the Balmis mission, is recorded as having arrived in Totonicapán from Chiapas and the Yucatán on November 4, 1804 [37]. Much to the chagrin of the governor of Totonicapán, Colonel Prudencio de Cozar, Pastor did not leave behind a supply of vaccine but proceeded instead directly to Guatemala City, from where both vaccine and instructions on how to use it were later disseminated [38]. The arrival of Pastor in Guatemala made it possible, from late 1804 on, for colonial authorities to undertake campaigns of vaccination against smallpox, campaigns in which the Indigenous population, because of its acknowledged vulnerability, was identified as the most important target group.
Regional committees were set up throughout Guatemala to supervise vaccination procedures, with medical personnel trained in the application of the new techniques paid as much as four pesos a day for their services [39]. One doctor active in the Sierra de los Cuchumatanes was Ignacio Ruiz, recorded in a document dated May 12, 1806 as having “a pleasant manner and style with the Indians, one that has resulted in the vaccination, by himself alone, of 10,127 persons in over fifty towns in the province of Totonicapán and Huehuetenango” [40]. By 1807, thanks to the efforts of Ruiz and others, over 3,400 natives had been vaccinated, the majority of them children aged fourteen years and under (Table 6). While this number, in an era not noted for its prompt engagement of medical innovations or progressive ideas, at first seem impressive, subsequent events did much to erode the beneficial impact of vaccination on Indigenous welfare. Resistance from wary sectors of the native population was always a problem, as was lack of cooperation among Spanish residents, some of whom were threatened with prison sentences for neglecting to attend to vaccination arrangements [41]. Fear of being pierced by a needle, apathy among the non-native elite, and problems related to vaccine supply and availability all contributed to periodic outbreaks of smallpox in Guatemala long after the Balmis-Pastor initiatives [42]. None of these outbreaks, however, had the profound impact of earlier epidemics, the result of which was sustained growth of the native population, despite local fluctuations. If Indigenous survival was not quite guaranteed, at least the intensity of one of its most lethal detriments had been significantly tempered.
Summing Up
The grief and despair of the afflicted, first and foremost, elicit our sympathy, but the above reconstruction of their fate is revealing from a scientific perspective. Of particular interest is the striking variation in the predicament of native communities when exposed to epidemic disease. While the smallpox epidemic of 1780–81 resulted in the loss of approximately 4,200 lives, or 15 percent mortality over the Sierra de los Cuchumatanes as a whole, death rates fluctuated significantly at the community level, from 8 per cent to 38 per cent. Variable local conditions best explain this pattern of differential mortality. Smallpox was fierce enough in 1780–81 to reduce the overall size of the region’s population; a similar decline, however, did not occur during another outbreak fifteen years later. It was therefore possible for the spatial impact of contagion to be discretely localized – that is, for sickness to affect some communities without necessarily reaching and levelling adjoining or surrounding ones. A regional population profile like the one pieced together for the Sierra de los Cuchumatanes, with downward and upward trends over time, is therefore likely to conceal fluctuations at the sub-regional (community or parish) level [43].
Not by “secret judgments of God” deemed to lie “beyond the reach of Man” did Spanish penetration of the Americas usher in Indigenous ruination [44]. A demographic collapse that, in all likelihood, was the most calamitous the world has known was brought about by the impact of disease on vulnerable, susceptible populations. In the Cuchumatán highlands, the magnitude and rapidity of native erasure conforms to a pattern now well established for other parts of Latin America. [45] A population of perhaps 260,000 on the eve of conquest, the approximate number who inhabited the region in the mid-twentieth-century, by 1680 had declined to around 16,000, a fall of more than 90 per cent over a period of 160 years. While disease-related mortality was most acute in the century and a half immediately following European intrusion, death due to Old World contagions was a characteristic feature of late colonial times as well.
A process of recovery that began toward the end of the seventeenth century continued throughout the eighteenth and nineteenth centuries. Population increase, however, was slow and sporadic because of persistent outbreaks of disease to which Indigenous inhabitants only gradually acquired immunity. Not until the beginning of the twentieth century did Maya peoples in Guatemala start to rise in size without interruption, a consequence of modern medical technology substantially reducing rates of mortality. By 1950, after a process of decline, recovery, and growth lasting over four hundred years, the native population of the Cuchumatán highlands reached a level equivalent to that which it may have been before the arrival of the Spaniards and their pestilential allies.
References list
- Anderson, Arthur J.O. and Charles E. Dibble, eds. and trans. [1555] 1978. The War of Conquest: How It Was Waged Here in Mexico, as Given to Fray Bernardino de Sahagún. Salt Lake City: University of Utah Press.
- Baxby, Derrick. 1981. Jenner’s Smallpox Vaccine: The Riddle of Vaccinia Virus and Its Origin. London: Heinemann.
- Benedictow, Ole J. 2004. The Black Death, 1346-1353: The Complete History. Woodbridge: The Boydell Press.
- Collins, Anne C. 1980. “Colonial Jacaltenango, Guatemala: The Formation of a Corporate Community.” Ph.D. dissertation, Tulane University.
- Cook, Noble David, and W. George Lovell, eds. [1992] 2001. “Secret Judgments of God”: Old World Disease in Colonial Spanish America. Norman: University of Oklahoma Press.
- Cook, Sherburne F. 1941–42. “Francisco Xavier Balmis and the Introduction of Vaccination to Latin America.” Bulletin of the History of Medicine 11: 543–60 and 12: 70–101.
- Cortés y Larraz, Pedro. [1768–70] 1958. Descripción geográfico-moral de la diócesis de Goathemala. Edited by Adrián Recinos. 2 vols. Biblioteca “Goathemala” 20. Guatemala: Sociedad de Geografía e Historia de Guatemala.
- Crosby, Alfred W. 1989. America’s Forgotten Pandemic: The Infuenza of 1918. Cambridge: Cambridge University Press.
- Dunn, Henry. [1829] 1981. Guatemala: or, the Republic of Central America, in 1827–1828. London: James Nisbet.
- Fenn, Elizabeth A. 2001. Pox Americana: The Great Smallpox Epidemic of 1775–82. New York: Hill & Wang.
- Few, Martha. 2010. “Circulating Smallpox Knowledge: Guatemalan Doctors, Maya Indians, and Designing Spain’s Smallpox Vaccination Expedition, 1780–1803.” British Journal for the History of Science 43 (4): 519–37.
- —. 2015. For All of Humanity: Mesoamerican and Colonial Medicine in Enlightenment Guatemala. Tucson: University of Arizona Press.
- Fuentes y Guzmán, Francisco Antonio de. [1690–99] 1967–72. Recordación florida, in Obras históricas de don Francisco Antonio de Fuentes y Guzmán. Edited by Carmelo Sáenz de Santa María. 3 vols. Biblioteca de Autores Españoles 230, 251, and 259. Madrid: Ediciones Atlas.
- Gil, Juan and Consuelo Varela, eds. 1997. Cristóbal Colón: Textos y documentos completos. Madrid: Alianza Editorial.
- Hidalgo, Joseph Domingo. 1797. “Descripción de la provincia de Totonicapán.” Gazeta de Guatemala (31 de julio, 6 de noviembre, and 13 de noviembre).
- Hopkins, Donald R. 1983. Princes and Peasants: Smallpox in History. Chicago: University of Chicago Press.
- Instituto Nacional de Estadística Guatemala. 2019. XXI Censo Nacional de Población y VII de Vivienda. Guatemala City. Accessed at: https://www.censopoblacion.gt/cuantossomos.
- IWGIA, International Work Group for Indigenous Affairs. 2019. Indigenous Peoples in Guatemala. Copenhagen, Denmark. Accessed at: https://www.iwgia.org/en/guatemala.html.
- Koch, Alexander, Chris Brierley, Mark M. Maslin, and Simon L. Lewis. 2019. “Earth System Impacts of the European Arrival and Great Dying in the Americas after 1492.” Quaternary Science Reviews 207: 13-36.
- León-Portilla, Miguel, ed. [1962] 1992. The Broken Spears: The Aztec Account of the Conquest of Mexico. Translated by Ángel María Garibay and Lysander Kemp. Beacon Press: Boston.
- Lovell, W. George. [1985] 2015. Conquest and Survival in Colonial Guatemala: A Historical Geography of the Cuchumatán Highlands, 1500-1821. Fourth Edition. Montréal and Kingston: McGill-Queen’s University Press.
- —. 1992. “‘Heavy Shadows and Black Night’: Disease and Depopulation in Colonial Spanish America.” Annals of the Association of American Geographers 82 (3): 426–43.
- —. [1995] 2019. A Beauty That Hurts: Life and Death in Guatemala. Toronto: Between the Lines.
- —. 2006. “Columbian Exchange: Disease.” In Iberia and the Americas: Culture, Politics, and History, edited by J. Michael Francis, vol. 1, 296–303. Santa Barbara: ABC-CLIO.
- —. 2020. “Columbus and Covid-19: Amerindian Antecedents to the Global Pandemic.” Americanía: Revista de Estudios Latinoamericanos 11, 4–31.
- Lovell, W. George and Christopher H. Lutz. 1996. “‘A Dark Obverse’: Maya Survival in Guatemala, 1520-1994.” The Geographical Review 86, 3: 398–407.
- Lovell, W. George and Christopher H. Lutz, with Wendy Kramer and William R. Swezey. 2013. “Strange Lands and Different Peoples”: Spaniards and Indians in Colonial Guatemala. Norman: University of Oklahoma Press.
- Libro Viejo de la Fundación de Guatemala y papeles relativos a D. Pedro de Alvarado. 1934. Prologue by Jorge García Granados. Guatemala: Tipografía Nacional.
- MacLeod, Murdo J. [1973] 2008. Spanish Central America : A Socioeconomic History, 1520-1720. Austin: University of Texas Press.
- McBryde, Felix Webster. 1946. “Influenza in America during the Sixteenth Century (Guatemala: 1523, 1559–1562, 1576).” Bulletin of the History of Medicine 8 (2): 296–302.
- Motolinía, Toribio de Benavente. [1541] 1979. Historia de los indios de la Nueva España. Mexico City: Editorial Porrúa.
- OHCHR, United Nations Human Rights Office of the High Commissioner. 2018. Report of the Special Rapporteur on the Rights of Indigenous Peoples: Country Visit to Guatemala. Accessed at: https://ap.ohchr.org/documents/dpage_e.aspx?si=A/HRC/39/17/Add.3.
- Razzell, Peter. 1977. The Conquest of Smallpox: The Impact of Inoculation on Smallpox Mortality in Eighteenth-Century Britain. Firle: Caliban Books.
- Recinos, Adrián and Delia Goetz, eds. and trans. 1953. The Annals of the Cakchiquels. Norman: Univeristy of Oklahoma Press.
- Remesal, Antonio de. [1619] 1964–66. Historia general de las Indias occidentales y particular de la gobernación de Chiapa y Guatemala. 2 vols. Biblioteca de Autores Españoles, nos. 175 and 183. Madrid: Ediciones Atlas.
- Schwartzkopf, Stacey. 2013 “Rural Castas, State Projects, and Ethnic Transformation in Western Guatemala, 1800–1821.” Ethnohistory 60 (4): 721–47.
- Shattuck, George C. 1938. Medical Survey of the Republic of Guatemala. Washington: Carnegie Institution of Washington.
- Smith, Michael M. 1974. “The Real Expedición Marítima de la Vacuna in New Spain and Guatemala.” Transactions of the American Philosophical Society, n.s. 64 (1).
- Swann, Michael M. 1980. “The Demographic Impact of Disease and Famine in Late Colonial Northern Mexíco.” Geoscience and Man 21: 97–109.
Notes
1. Benedictow 2004 and Crosby 1989.
2. Koch et al. 2019 model the “great dying” at 54.5 million, a mid-point between a low of 39 million and a high of 72.4 million.
3. See Lovell 1992 and 2006, and Cook and Lovell [1992] 2001 for extended discussion.
4. Guatemalan censuses are notoriously unreliable, the manner in which they are carried out riddled with all sorts of methodological and procedural problems – which calls for caution and prudence when consulting and citing them. In percentage terms, for example, the 2018 census computed a self-identified Maya tally of 41.7 percent (Instituto Nacional de Estadística Guatemala 2019) but two non-government sources reckon the Maya count at closer to 60 percent (OHCHR 2018 and IWGIA 2019). For indications of government manipulation that consistently under-estimates the Maya percentage of the national population, see Lovell and Lutz 1996.
5. See Lovell [1985] 2015, upon which this contribution is based, and Lovell [1995] 2019 for elaboration.
6. Lovell [1995] 2015, 19. The 1973 census, carried out before the peak mayhem (1978-1983) of the Guatemalan armed conflict, and the 2002 census, undertaken six years after the signing of a peace accord, are regarded as two of the more reliable national surveys, hence their being drawn upon with respect to numbers, population increase, and ethnic ratios and percentages.
7. Gil and Varela 1997.
8. Motolinía [1541] 1979, 13–140; León-Portilla [1962] 1992; Anderson and Dibble [1555] 1978.
9. Shattuck 1938, 40–1; MacLeod [1973] 2008, 19, 98.
10. MacLeod [1973] 2008, 40. Shattuck 1938, 41, on the advice of France V. Scholes, dates the epidemic to 1521. McBryde 1946, 301–2 suggests that the date should be 1523 and contends that the disease in question was a strain of influenza.
11. Recinos and Goetz 1953, 115. Shattuck 1938, 42 quotes Fuentes y Guzmán (1690–99) as stating that, before Spanish intrusion, Guatemala was densely settled until smallpox and measles spread among the native population “like fire in dry grass, destroying entire cities of thousands of inhabitants.”
12. Pedro de Alvarado to the Crown, September 1, 1532, in Libro viejo 1934, 282.
13. For insightful discussion of the emergence of casta populations in the region, their numbers, places of residence, and livelihoods, see Schwartzkopf 2013. Only in Cuilco, Chiantla, Huehuetenango, and Santa Ana Malacatán did Spaniards and Ladinos become noteworthy elements of the local population. For the year 1779, see Archivo General de Centro América (hereafter AGCA), legajo (hereafter leg.) 6097, expediente (hereafter exp.) 55507, folio 51; for the year 1803, when some five hundred casta families are documented, see AGCA A1.44, leg. 6106, exps. 55866, 55867, and 55892.
14. AGCA, A1, leg. 6112, exp. 56104 and A1, leg. 6112, exp. 56108. For the hemispheric dimension of this outbreak of smallpox, see Fenn 2001, whose tracking of the disease and the destruction it caused is masterly.
15. AGCA, A1.44, leg.6097, exp. 55507, folio 27 verso.
16. AGCA, A1.44, leg. 6097, exp. 55507. Hopkins 1983, 8–9 notes that smallpox tends to spread “more rapidly in the winter months in temperate climates and during the dry season in tropical climates.” His observation applies to some extent to the Cuchumatán chronology, which indicates a more rapid diffusion of infection west to east in the dry season and a slower diffusion north into higher elevations once the annual rains had begun.
17. AGCA, A1.44, leg. 6097, exp. 55507, folio 34.
18. AGCA, A1.44, leg. 6097, exp. 55507, folio 49, “Estado general que manifiesta los que fallecieron durante la epidemia de viruelas en los pueblos de la alcaldía mayor de Totonicapán y Huehuetenango durante el año 1780” (1781).
19. Such high mortality among children is not surprising, as they constituted the majority of the non-immune population. Regeneration of non-immune populations allowed smallpox to occur in cycles of seven or eight years. See Swann 1980, 105 for elaboration.
20. AGCA, A1.44, leg. 6097, exp. 55507, folio 26.
21. For discussion of these same variables operating in a Mexican context, see Swann 1980, 97–109.
22. AGCA, A1.44, leg. 6097, exp. 55507, folios 46 verso and 47. The original states “por punto general se mandó cuidar y soccerer a los indios de los fondos de sus comunidades”.
23. AGCA, A1.44, leg. 6097, exp. 55507, folios 46 and 47.
24. AGCA, A1.44, leg. 6097, exp. 55507, folios 35 and 36.
25. Asturias 1958, 88; see also Shattuck 1938, 42. Few 2010 documents the practice of inoculation in meticulous detail during the 1780 epidemic, noting the prominent role played in it by José Flores, a “medical physician” who “later became head of the Audiencia de Guatemala’s Royal Protomedicato and chair of medicine at the Universidad de San Carlos”. Flores and a team of assistants trained in the art of injecting a person with live smallpox matter – which, if successfully undertaken, induced immunity to the disease – concentrated their activities in and around the new colonial capital (the present-day Guatemala City) founded only a few years before the outbreak. See Few 2015 for further, even more incisive and well-documented discussion.
26. Hidalgo 1797, writing in the Gazeta de Guatemala of July 31.
27. AGCA, A1.47, leg. 385, exp. 8012.
28. Hidalgo 1797, writing in the Gazeta de Guatemala of July 31. His words in the Spanish original run: “En los años inmediatos de 1795 y 1796, los pueblos confinantes con la provincia de Chiapa [...] se infestaron del terrible contagio de las viruelas, peste devoradora, y causa principal de que este Reyno, en 275 años que lleva de conquistado, no haya tenido el debido incremento la propagación, pues destruye los renuevos, y apenas dexa el diezmo para la subsistencia de las poblaciones; pero esta vez, a esfuerzos del Muy Ilustre Señor Presidente Capitán General del Reyno Don José Domás y Valle, se aisló el contagio [y] se entabló la inoculación y se sofocó la peste en medio de su mayor ardor”.
29. AGCA, A1.47, leg. 385, exp. 8012, folios 2 recto to 3 verso.
30. AGCA, A1.47, leg. 192, exp. 3922; A1.4, leg. 61105, exp. 55836.
31. AGCA, A1.47, leg. 192, exp. 3922.
32. AGCA, A1.4, leg. 6105, exp. 55836.
33. AGCA, A1.47, leg. 192, exp. 3922. “Han venido y vienen sin cesar”, the official noted, “gentes de todas partes”.
34. Baxby 1981, 38–88, 179–96; Razzell 1977, ix.
35. The designation, “feliz descubrimiento inglés” in the original, comes from a document in AGCA, A1.47, leg. 4027, exp. 31012. For extensive discussion of the Spanish medical mission, see Cook 1941 and 1942, and Smith 1974. Both researchers worked with sources housed in the Archivo General de la Nación in Mexico City. Smith, however, also had microfilm access to two voluminous legajos (Indiferente General 1558A and 1558B) housed in the Archivo General de Indias in Seville. Their contents have more recently attracted the attention of Few 2010 and 2015, who delves into them most diligently.
36. Cook 1941–42, 545–46.
37. AGCA, A1.4, leg. 6091, exp. 55306, folio 160.
38. AGCA, A1.4, leg. 6091, exp. 55306.
39. AGCA, A1.47, leg. 193, exp. 3939.
40. AGCA, A1.47, leg. 193, exp. 3939 The original attributes to Ruiz “buen modo y estilo con los indios, de que resulto haber vacunado por su mano 10,127 personas”.
41. AGCA, A1.47, leg. 2162, exp. 15558; A1.47, leg. 385, exp. 8012; and A1.47, leg. 191, exp. 3905.
42. See, for example, AGCA, B.82.3, leg. 1095, exp. 24046; B.82.3, leg. 1095, exp. 24048; B.82.3, leg. 1095, exp. 24050; and B.82.3, leg. 1095, exp. 24069, all of which concern an outbreak of smallpox throughout Guatemala between 1829 and 1831. The Kaqchikel región was particularly hard hit, especially San Juan Comalapa and surrounding communities. More isolated outbreaks are recorded for San Miguel Totonicapán in 1824 (AGCA, B.68, leg. 98, exp. 2694); San Antonio and Santa Ana Huista in 1825 (AGCA, B. 99.2, leg. 1412, exp. 32999); and the Verapaz in 1826 (AGCA, B82.3, leg. 3587, exp. 81954). Dunn [1829], 1981, 151–3 also comments on problems related to the eradication of smallpox in Guatemala.
43. For an illustration of this tendency, see Collins 1980, 48–58, which indicates that data for Jacaltenango do not fit the general Cuchumatán pattern. For colonial Guatemala in its entirety, see Lovell and Lutz with Kramer and Swezey 2013, 173–248.
44. Pedro de Liévano’s divine attribution, culled from testimony of his in the Archivo General de Indias (Guatemala 10), in the original runs: “En lo que toca morirse los indios e ir en dismunición son juicios secretos de Dios que los hombres no los alcanzan [pero] lo que este testigo ha visto en el tiempo que ha estado en estas provincias es que desde la provincia de México han venido tres o cuatro pestilencias con las cuales ha venido la tierra en grandísima disminución”.
45. See Lovell 2020 for discussion of the chronology and impact of disease outbreaks in Brazil, Ecuador, Guatemala, Hispaniola, Mexico, and Peru, in which regional findings are set, historically, in hemispheric and global context.

 Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
International License 2004- 2026
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
International License 2004- 2026
